
Many Temporomandibular Disorders (TMJ, TMD) are still best treated with conservative therapy.4/23/2018 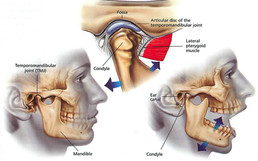 In May of 1988 I wrote a series of articles for the Mobile Press Register concerning causes and treatment for Jaw Disorders. Many of the treatment options discussed are still used today. Conservative therapy is usually effective and surgery is rarely needed to resolve most of these conditions. The first article discusses the causes and the second covers treatment options. I have scanned the articles and posted them on this blog as a reference. 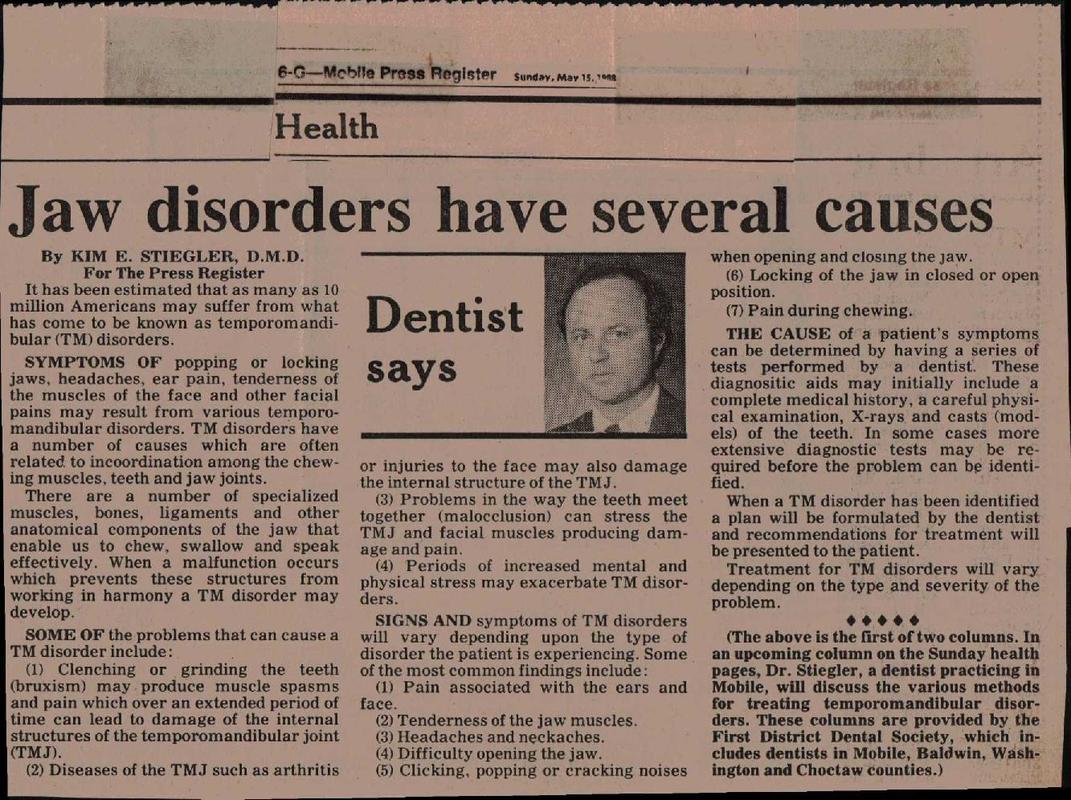 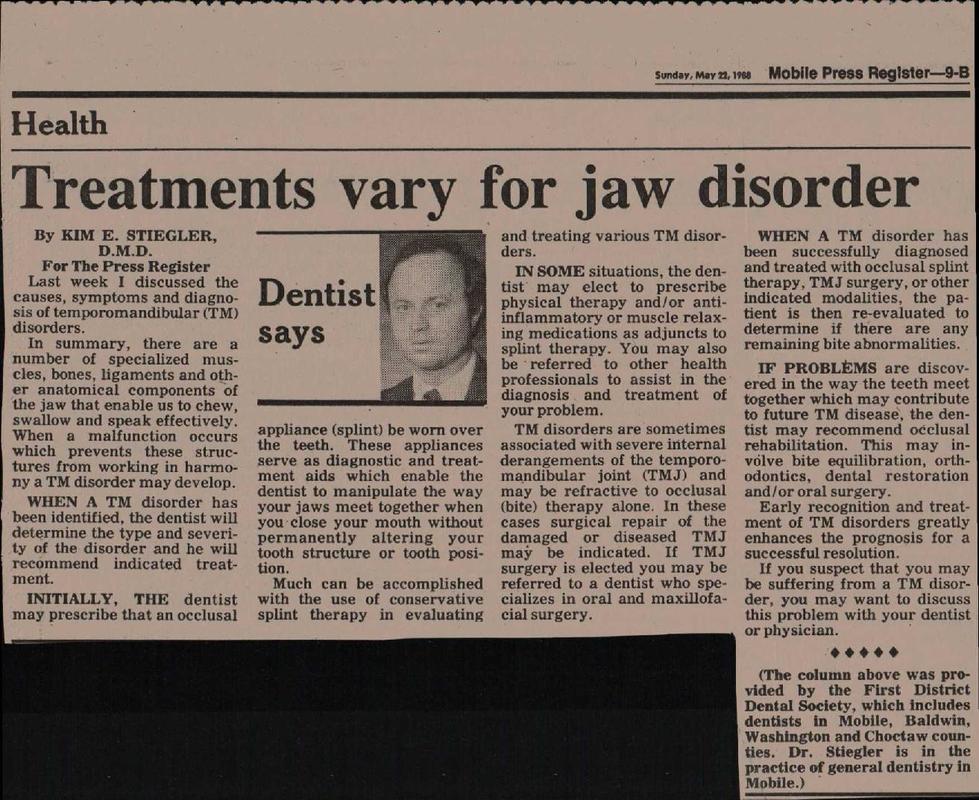  Click image for more information Click image for more information Dental care is often put off because of concerns about the cost. Many people delay having preventive care or treating dental conditions until they can obtain Dental Insurance. The reality is that good Dental Care can be affordable with or without Dental Insurance. Dental Insurance premiums in many cases exceed the amount of dollar benefits that are actually spent by the Insurance Company on dental services. If your employer offers Dental Insurance as a tax exempt benefit it can certainly help offset some of the expenses of dental care especially preventive care. Purchasing individual Dental Insurance with your earned after tax dollars can often cost more than the actual benefits received and can also restrict your access to a limited number of Dentists. Having your teeth examined regularly can enable you to prevent and treat dental problems early at a significant decrease in cost. Even if you have put off Dental Treatment for a long time and you suspect that you need a lot of care, it is important to have this seen and evaluated by a Dentist. You may be surprised to learn that there may be some affordable options to treat your problems. Speak to your Dentist about your concerns about cost. Often there are conservative alternatives to treating your immediate needs allowing time for you to phase in more extensive treatment over time while alleviating your immediate pain and cosmetic concerns. Expensive Crowns can sometimes be avoided by using less expensive esthetic bonded fillings. Early dental caries can often be arrested, eliminating the need for fillings.  Click on image for more information If you have already been to a Dentist and have been told you need a lot of expensive care it may be in your best interest to seek a second opinion from another Dentist. You may find another Dentist who can offer you some conservative cost effective ways to handle your Dental needs.
 There are a number of studies that have revealed an association between Periodontal Disease (Gum Disease) and Heart Disease. A direct cause and effect has not been proven but there are indications from research that Periodontal Disease increases the risk of Heart Disease, Stroke, Cancer, Diabetes and other health problems.  Studies show that half of all Americans and 70% over the age of 65 have Periodontal Disease. Risk factors include: Genetics (some people are more susceptible), Age, Smoking, Stress, Medications, Clenching or Grinding your teeth, other Systemic Disease, Obesity, and Poor Nutrition. 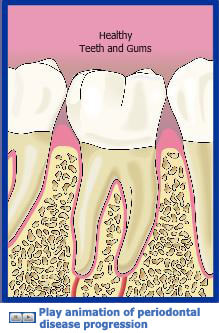 Click on picture to view animation from the AAP website Click on picture to view animation from the AAP website Periodontal Disease is a disease of supporting structures of the teeth which can lead to infection, loss of bone and eventual tooth loss.  Click on picture for VIDEO of a Periodontal Exam from the ADA Click on picture for VIDEO of a Periodontal Exam from the ADA Periodontal Disease can only be diagnosed by a Dentist or Dental Hygienist. In our office we perform a periodontal evaluation during your Dental Examination when you have your teeth cleaned which includes probing your gums for signs of periodontal disease. The good news is that Periodontal Disease can be treated and prevented but it is important that you have your teeth cleaned and examined by a dental professional on a regular basis. Periodontal Disease can go undetected and lead to infection and loss of teeth if it is not diagnosed early. The American Academy of Periodontology lists the signs of periodontal disease as the following:
 Click for video on tooth decay from the American Dental Association Have you been told you have lots of new cavities (aka: caries) that you did not expect! Dental caries are caused by bacteria that live in our mouths that stick to our teeth. When we consume sugar containing substances this causes these bacteria to produce acids that decay our teeth. During the Christmas Season we tend to consume more sugary foods but we also are exposed to more cold viruses and the associated coughs that come with them. Cough drops can contain sugar and because they remain in our mouths for extended periods of time they can be a significant cause of dental caries. It is important to note that even small quantities of sugar can cause tooth decay if they are in contact with our teeth for a long time. So try to minimize the amount of sugar containing foods and beverages that you consume in between meals. If you use cough drops or breath mints make sure they are sugar free. If your dentist tells you that you have a lot of new cavities look for new sources of sugar that you may be consuming and try to minimize your exposure. If you are seeing a Dentist for the 1st time and you are told you have a lot of cavities that you did not expect you may also want to consider a second opinion.
  Intravenous Sedation (IV) is a method for administering sedative medications directly into the bloodstream. This allows for the sedative medications to be titrated in a safe and effective manner for each individual patient's needs. Unlike oral sedation the effects of the medication are achieved quickly and predictably and can be better adapted to the tolerance of each patient's specific needs.  Sedation in Dentistry has a long history of safe and effective use. Modern technology allows us to more carefully monitor patients during procedures and combined with newer drugs and techniques we can achieve even better safety and comfort for our patients who have anxiety about receiving Dental Care. I wrote the article below which appeared in the March 16, 1986 edition of the Mobile Press Register. It described methods for controlling Dental pain and anxiety that we still use today.   A Dental Microscope allows for very high magnification and better illumination. Higher magnification can enabe a Dentist to provide more precise and conservative care. With the combination of a high definition camera it also allows the Dentist to project an image on a screen so the patient and assistant can watch the procedure and digital images can be captured for better communication.  Click on this link to watch a video that shows the capabilities of the Dental Microscope and how it can help a Dentist provide better more conservative care: Microscope Video
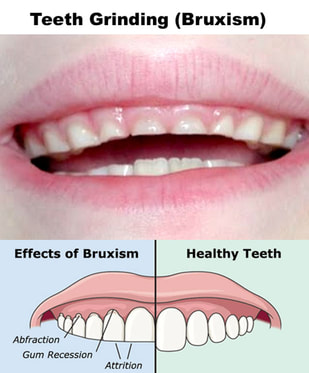
 Teeth Grinding , also known as Bruxism , can occur as a habit while you are awake or as an unconscious behavior while you are asleep. Nocturnal Bruxism usually occurs during a phase of sleep where the patient has no recall of the activity.  This is often a very intense activity that can lead to severe attrition and fracture of teeth as well as Temporomandibular (TMJ) Disorders.  Prevention of damage from nocturnal bruxism is often accomplished with occlusal appliances sometimes referred to as Splints or Nightguards  It is important to see a dentist who is trained in treating TMJ Disorders (TMD) to evaluate your condition and deliver a properly designed and equilibrated splint. Improperly constructed and adjusted appliances could lead to pain and further damage to your teeth and jaws.  If you are aware of clenching or grinding your teeth while you are conscious it is important to note that your teeth should only touch together while you are chewing or momentarily when you swallow. Any other tooth contact is considered parafunctional and can lead to problems.
Evidence of Nocturnal Bruxism could include soreness , pain, and/or popping in your jaws, teeth attrition or fracture of teeth from unknown origins, or wedge shaped defects and recession at the gum line of your teeth (abfraction lesions).  If you suspect that you have this problem it is important to discuss this with your Dentist. Early diagnosis and treatment can prevent more serious damage to your teeth and jaws and may help you avoid extensive and expensive teeth rehabilitation.
 If you have an emergency or you need to get in for an appointment, your Dentist should be available to help you. Many Dental Emergencies need immediate attention and it is important that you are an established patient of record with a Dentist that is available when you need him even if it is after office hours or on a weekend. You also want your Dentist to make arrangements for another Dentist to cover his emergencies when he is unavailable.  You should not have to wait a long time for an appointment. You want your Dentist to be able to see his established patients for routine care within a reasonable length of time.  Your Dentist cannot be an expert in every area of Dental Care and should make referrals to appropriate Dental Specialists when it is in your best interest. If you need the care of a Dental Specialist you want your Dentist to be your advocate and communicate your needs to the specialist and assist you in getting a timely appointment.
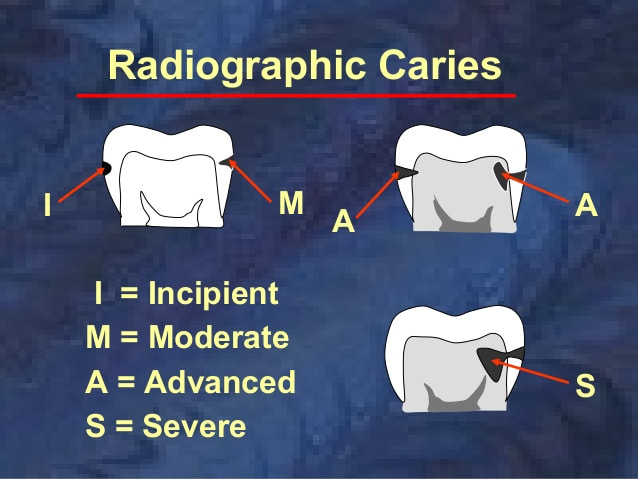
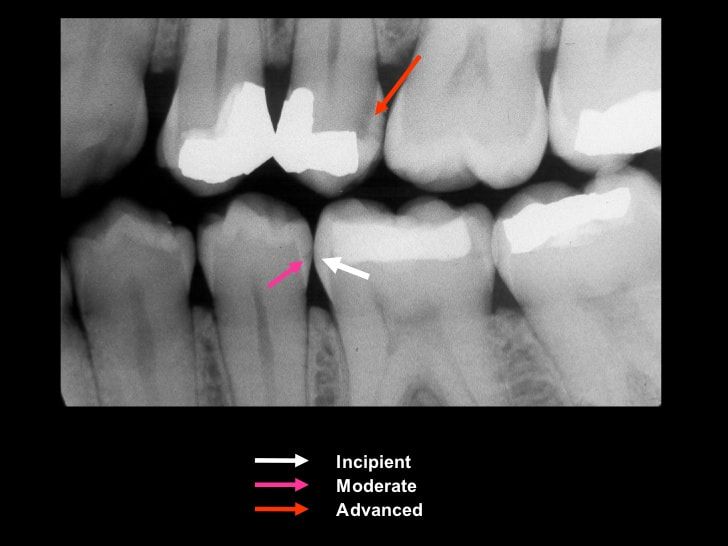
Some early, incipient cavities between teeth can actually repair themselves. If interproximal (between teeth) dental caries (decay) is discovered in its early stages on a dental radiograph (x-ray) it can often be arrested if the cause (e.g., chronic sugar consumption) is removed and the patient exercises good oral hygiene. The use of prescription strength topical fluoride and other remineralizing agents can also help facilitate repair and prevention of future cavities. Most dentists agree that these early lesions should not be restored to avoid unnecessary expense, discomfort and damage to teeth. When a carious tooth is restored, the tooth will become weakened and more susceptible to future fracture. It is important that the patient not miss his regular cleanings and examinations so these areas and his overall dental health can be monitored. If it is discovered later that one of these early cavities have decayed beyond the degree that they can remineralize then they can usually be restored with no additional loss in tooth structure compared to restoration when they were first noted. The decision to restore a tooth with decay is made by your Dentist based on your particular circumstances. Some Dentists are more aggressive and elect to restore these lesions so if you are concerned about this you may want to consider a second opinion.
|


 RSS Feed
RSS Feed